Lupine Publishers- Biostatistics and Biometrics Open Access Journal

Abstract
In
2001, a survey of the veteran members of the British Korean War Veterans
Association was conducted with support from the Royal British Legion. As a part
of this survey, the present inquiry addresses the relationship between older
combatant and noncombatant veterans’ levels of combat exposure, their losses
and Gains in life and current psychological symptoms. Nine hundred and
ninety-four British Korean War veterans provided data for four measurement
scales: The Combat Exposure Scale (CES); the Losses from life scale and the
Gains from life scale, and the Impact of Event Scale (IES). Significant
positive correlation effects were found between life losses (but not life
gains) with and between the CES and the IES. Combatants had an overall score on
the IES that clearly exceeded its recommended cut-off level but notably the
score for non-combatants was just approaching the cut-off, indicating that some
of them were also experiencing psychological symptoms just from being in the
war zone. Although it is now some 65 years since the cessation of fighting in
1954, the findings seem to suggest that their life losses are not positively
influenced by their life gains, rather they appear to co-exist.
Introduction
Hickey
(1999) states that the Korean War (KW) of 1950-54 was the first serious
conflict of the Cold War and a major test of the United Nations with troops
sent from 16 countries [1]. Some 100,000 personnel from the United Kingdom (UK)
served in the Korean War. Two-thirds of the land-based troops were National Service
men and Reservists (mandatorily recalled civilians having served in World War
II [WWII]) and the remainder were Regular soldiers. Over the war’s course,
there were periods of both fierce fighting and tense stalemate, conducted in an
inhospitable terrain with a harsh climate of permafrost in winter and high
temperatures in summer. Some 1,106 British troops were killed in action, more
were injured, and 1060 were taken prisoner or were missing. Aside from military
action, many witnessed the plight of large numbers of Korean refugees who had
fled from North to South ahead of the advancing communist North Koreans backed
by China [1].
Review
of the Literature
Military
service is regarded as exerting an important influence upon veterans’ lives [2]
yet the potential for adverse effects from combat exposure has been described
as a ‘hidden variable’ in the lives of older men [3]. These effects can lie
dormant for decades, only to re-emerge later in response to other adverse
changes in roles, relationships, and mental and physical health [4,5]. Much of
war-based literature focusses upon adversity and/or human vulnerability as
outcomes from participation in warfare and in general, combatants are shown to
be those most prone to post war anxiety, depression and Post Traumatic Stress
Disorder (PTSD) [3,6,7]. Participation in warfare can have positive as well as
negative effects [3,7,8]. These have been referred to as: losses and gains [7],
or post-traumatic or stress-related growth or benefit [3,9]. Reasons why some people
show benefit from a stressful experience while others become debilitated by it
has been studied through measurement of personal attributes such as: perceived
optimism and pessimism [10]; locus of control [11]; self-esteem and
selfefficacy [12], and increased resilience [7,13]. In a longitudinal study of
college students that used a pre-tested measurement scale, stress–related
growth was associated with the level of religious belief; positive coping
strategies; the number of recent positive life events, and social support
satisfaction [14].
Several
studies have shown that combat exposure and other adverse experiences can lead
to negative psychosomatic outcomes for veterans such as PTSD, that may be short
term or long term [15- 17] and may continue into late life [7,18]. Increasingly
the complex study of the impact of war-service upon the lives of participants
includes consideration of childhood and family histories [19]; pre, during and
post deployment war factors [20], and other intervening life events [21]. The
role of post war social support [22] and the effects of the quality of the
homecoming experience in terms of unmet expectations are also believed to be
influential factors in post war mental health [23] and include not only the
home-based family’s support but also that from the workplace [24]. A further
consideration for this enquiry is to contribute to fleshing out the knowledge
of the long-term effects on UK KW veterans as a distinct cohort. For, often
researchers have often placed KW veterans in mixed samples with those of WWII
on the basis that both Wars’ veterans are in their ‘late life’. Although some
research shows similarity of responses between veterans of different wars, it
can be argued that there is sufficient evidence for the KW veterans to stand
alone. For example, when veterans of the KW, the Vietnam War (VW) and WWII were
compared, although the severity of psychiatric symptoms was primarily related
to severity of combat experience and independent of the theatre of war, the
frequency with which the symptoms appeared differed between the wars’ cohorts
[15]. Furthermore, in other research by McCranie and Hyer (2000) comparing the
severity of PTSD symptoms in KW and WWII veterans, they found that the KW
cohort had more pronounced symptoms, even after controlling for confounding
variables such as age and different levels of combat exposure [25].
In
general, returning US KW veterans were welcomed back home but as UK society was
still war-weary from WWII, there was little interest in this far away war or
its veterans. UK media reporting was low, particularly for returning troops who
were often treated with indifference [26]. For this reason, it is often
reported as ‘The Forgotten War’ and anecdotally its ‘forgotten’ veterans
believe themselves to be ‘different’ from other wars’ veterans. Now well into
their third age, US research with WWII and KW US veteran participants [27]
shows that older combatant veterans with PTSD are associated with increased
morbidity. Ikin et al. [28] similarly found an association between combatant
war service, anxiety, posttraumatic stress disorder (PTSD) and depression in
7525 surviving Australian male KW veterans in comparison with a community
group. In terms of life gains and losses, other authors suggest that traumatic
stress poses both risks and benefits but the positive benefits from military
experiences can counter the negative sense of loss that is seen to accompany
combatants [8].
Combatants
(unsurprisingly) are shown to be those most prone to post war anxiety, depression
and PTSD [3,7]. However, whilst there is plenty of evidence supporting the
argument that heavy exposure to combat is a strong predictor of psychiatric
symptoms, what is less clear is if simple exposure to a war zone can in some
circumstances also be stressful. Relatively little attention has been paid to
the distinction between the setting where combat takes place and the combat
activities themselves. Accounts of the KW certainly indicate that even for
non-combatants, conditions could be very stressful indeed. For example, there
was the constant apprehension even after the war entered its ‘standoff’ phase
that a counter-surge might be imminent. Given the extremely labile conditions
of the first stage of the war, this was a reasonable paranoia and not helped by
UK troops reportedly not being adequately clothed to protect them from cold
injuries in the sub-zero winter climate in the early part of the War [29].
Methodology
Sample Selection and Method
The
UK KW veteran participants were recruited opportunistically through the British
Korean Veteran Association. A preliminary article to explain the intended
survey was published in the members’ magazine. In the subsequent issue, the
questionnaires, completion instructions, and pre-paid return envelopes to the
researchers were inserted in 4000 magazines with a request for anonymous
completed returns to the researcher within a four-week period.
Materials and content
The
questionnaire sought to establish personal and military characteristics
including: age; marital status: type and length of service, rank, where service
took place, role in warfare and duties; receipt of war pension if applicable; a
health checklist, and current levels of social and health care support. The
intensity of war experiences was measured using an adapted version of the
Combat Exposure Scale (CES) [30] with 9 ordinal items with values of 1 no
exposure through to 6. heavy exposure. The intensity of losses and gains from
war-time experiences in post war life was measured by the 14 item losses scale
(LS) and 14 item gains scale (GS) [7]. Each item had the ordinal values of 1.
Not at all through to 4. A lot [7]. The final measure, the Impact of vent Scale
(IES) [31] determined levels of intrusion and exclusion of thought arising from
the respondent’s experiences of the KW and had 15 items with the ordinal values
of 1. not at all through to 4. a lot.
The key objectives for the inquiry
For
the purpose of this article, the following three objectives were set to guide
the analysis:
A.
To observe and compare the veterans’ levels of subscription to individual items
in the life losses and gains scales.
B.
To identify the significance of correlations effects between the KW veterans’
levels for combat exposure, their life Losses and Gains, and presence of
psychological symptoms in the Impact of Event Scale.
C.
To establish the significance of differences between the combatants with
non-combatants using t test on the same four scales as above in ii].
Results
Return Rate and Data Management
The
postal survey, conducted in 2001, resulted in 1009 returned questionnaires of
which 15 were so poorly completed that they were discarded as unreliable. Of
the remaining 994 returned questionnaires attention was drawn to the high
number of missing values predominantly in the psychology-based scales (the IES
and CES). For example, 76 veterans had missing values in the completion of the
CES and 116 in the IES (missing could be due to non-completion of a whole
scale’s items or more frequently non completion of scale’s single or multiple
items). In contrast, other dichotomous more factual questions such as combat
status, there were in general only 20 veterans or fewer missing values. Reasons
for this are suggested later in the conclusions. The above anomalies required a
pragmatic approach to reduce complexity whilst facilitating reliable
statistical outputs. Hence, the scales’ data were standardized to n=994 before
statistical comparisons were made, using the SPSS facility for
computer-generated missing data replacement. It is of note that there were
minimal differences in a pre-test using the same tests (correlation and t test)
between the outputs from the original data with those manipulated to replace
missing data and no difference was found in their respective levels of
statistical significance.
Sample Characteristics
The
994 participating veterans represented some 1 in 4 of the total BKVA
membership. Of these, their mean age in Korea was 22 years and at the time of
the survey their mean age was 70. Most were: in the army; land-based; male;
undertaking National Service and of other ranks. Of the 994 participants, 504
were combatants and 490 were non-combatants.
Veterans Subscription to Life Losses and Gains Scales’ Items
The
responses to the 14 items in each of the two scales for losses and for gains,
respectively, were reviewed to identify items that were the most frequently
subscribed to or of other comparative interest between the two groups
(combatants and non-combatants). In work by Aldwin et al. [3], these positive and
negative life span appraisals have been related to the diagnosis of veterans
with PTSD symptoms in later life. The mean scores are given for combatants and
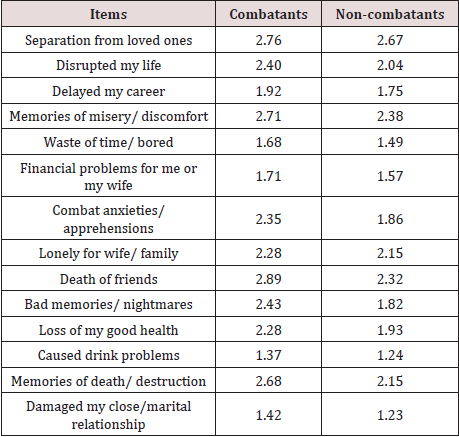
non-combatants in Table 1 for losses and in Table 2 for gains. As shown in
Table 1, combatants’ mean scores for losses items were consistently higher than
those for non-combatants. The most marked differences where combatants had
notably higher mean scores than non-combatants were in the following 7 numbered
items: Disrupted my life [2]; Memories of misery/discomfort [4]; Combat
anxieties/apprehensions [7]; Death of friends [9]; Bad memories/nightmares [10]
; loss of my good health [11] and Memories death/ destruction [13].
Table
1: Mean values for life losses by
combat status.
Table
2: Mean values for life gains by combat
status.
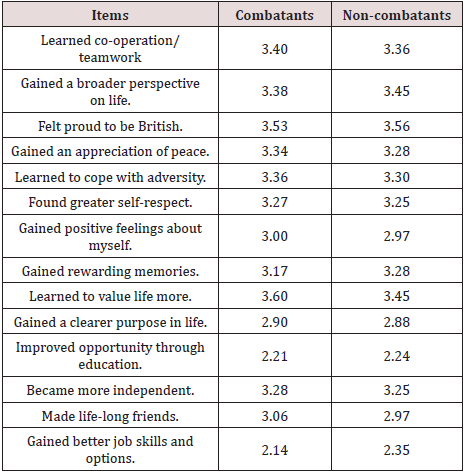
In
contrast, as shown in Table 2, the mean scores for life gains items for both
combatants and non-combatants were higher than those for losses and the
differences between the two groups’ sets of mean scores were much smaller than
those for Losses. This suggests that both groups perceived that the kW
contributed more gains to life than losses. Non-combatants had notably higher
mean scores than combatants for the following gains numbered items: gained a
greater perspective on life [2]; gained rewarding memories [8]; gained better
job skills and options [14]. Conversely, combatant gains at a notably higher
level than non-combatants comprised only one item: Learned to value life more
[9].
Correlation Effects
The
second stage of the analysis sought to determine the correlation effects
between losses and gains mean scores with and between those of the CES and IES.
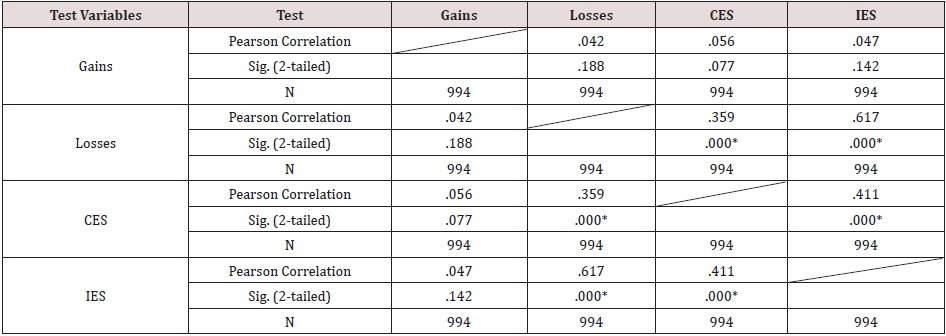
The correlation matrix is shown as Table 3. There were no significant
correlation effects between the gains score with that of the CES, the IES, or
losses. However, significant positive correlation effects are shown for the
losses score with the CES (p<0.01)
and the IES scores (p<0.01),
respectively. The observed positive effects indicate that veterans with higher
scores on losses from life were significantly associated with higher scores on
the CES (indicative of higher combat exposure) and on the IES (indicative of
higher levels of intrusion and avoidance of thought).
Table
3: Correlation effects for Losses and
Gains Scores with IES and CES scores (n=994). *Correlation is significant at
the 0.01 level (2 tailed).
Independent t-test
To
identify the significance of the difference between combatants’ and
non-combatants’ scores on each of the four scales, first the group means were
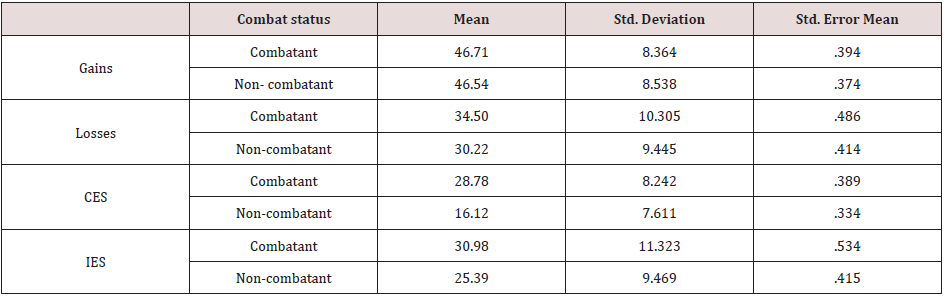
reviewed, as shown in Table 4. The mean scores for life gains were similar
between the two groups but as expected the means for life losses were higher
for combatants than non-combatants. It is of note, that the IES cut off score
for the presence of psychological symptoms is set at 26 and above and whereas
combatants clearly exceeded this with a mean score of 30.98, non-combatants
were nearly approaching the cut off with a score of 25.39. This suggests that
as some noncombatants must have had scores above the cut-off, just being under
the combat zone’s conditions appears to have been sufficient to produce
psychological symptoms later in life in them too. When independent t-tests were
undertaken, the difference between the combatant and non-combatant groups’
respective mean scores was significant for life losses (t=6.706, df=918.93, p<0.01), but not for life gains (p>0.05). Furthermore, the differences between these two
groups’ scores were significant for the CES (t=24.73, df=921.89, p<0.01)-and the IES (t=8.27, df=878 52, p<0.01), respectively. Thus, combatants were more likely than
non-combatants to have had greater exposure to combat, higher levels of losses
from life and to be experiencing psychological symptoms stemming from their KW
war service.
Table
4: Group statistics for Losses and
Gains: Combatants and non-combatants mean scores.
Limitations
The
article provides findings based on a large participant sample of British KW
veterans. Arguably as a community–based sample, it avoids some of the bias
problems that may arise when sampleselection is based upon veterans as patients
already presenting with clinical levels of a psychiatric disorder. Furthermore,
it is recognized that at this distance in time from the KW, asking for
retrospective judgements from the participants may involve bias through
exaggeration or diminish memory. However, other authors in a comparative study
of US military men’s present appraisals of World War II with those recorded
after it, found that the former significantly predicted the latter [32]. A
further issue concerns the representativeness of the participant sample. In
this, it is possible that by only attracting responses from a quarter of the
target KW veterans, there could be bias towards those with an ‘an axe to grind’
but there was no evidence suggesting this form of bias in the comments. Indeed.
the poor level of completion of psychological scales would suggest that the
survey could have underestimated rather than overestimated the extent of the
psychological problems being experienced by the KW veterans and some receiving
the questionnaire may have been too distressed to complete it.
Discussion
Although
life gains from wartime experiences were perceived mostly at similar and higher
levels than life losses by combatants and non-combatants, there were
differences in emphasis in individual items. Non-combatants tended to perceive
their war experiences as having offered opportunity to gain education and
skills, whereas combatants perceived their life gains as growth in personal
resilience and valuing life, both probably because of surviving the war. Losses
on the other hand for combatants reflected the miseries of warfare in terms of
death and destruction. There is no evidence to suggest combatants heightened
level of current psychological symptoms have been positively influenced by
their life gains, as suggested by other authors [8]. Rather, their life losses
and gains seem to co-exist without interaction. (Reasons for this will be made
clearer when the qualitative interview data is published later.
A
sizeable number of KW veterans living in the community were found to have
psychological symptoms that must (at the least be marring) their quality of
life. However, what is of interest is that, psychological distress has arisen
in non-combatants as well as combatants just from being in the war zone and
being exposed to the extremes of the climate, appalling living conditions and
loss of friends. Although some overall similarity between these present
findings with earlier studies of mixed KW with WW11 veteran samples [2, 3-5],
it also supports the case for KW veterans to be studied as a stand-alone
sample, if such subtle differences are to be clearly identified.
The
emergence of PTSD symptoms in older veterans has been noted in the US
literature for some years [32] particularly when in tandem with the onset of
age-related morbidities or exposure to traumatic news events triggering dormant
trauma-induced syndromes [33]. From a UK perspective, in a mixed veteran sample
(WWII with KW veterans), Hunt and Robbins, (2001) found that almost a fifth of
the sample scored above the threshold on completion of the General Health
Questionnaire and the IES [34]. Their results collectively indicate the
presence of traumatic long-term effects of combat exposure in older KW
veterans. However, without clinical diagnoses, PTSD could not be confirmed, as
is the case with the present study. Similarly, the interesting question posed
by Spiro et al (1991) as to whether PTSD in older veterans occurring after
their exposure to combat is following the true course of the disorder or is it
a consequence of a failure to recognize and treat the disorder [35], also
cannot be addressed by the present study. However, the findings reinforce the
view that although combat exposure in the KW is particularly associated with
long-term psychological distress in later life, the non-combatant’s exposure to
the conditions of the warzone alone also seems to produce adverse effects long
after the event.
Finally,
the apparent reluctance of a high number of these veterans to fully complete
psychology-orientated scales perhaps uncovers a long-standing cultural dislike
of inquiry that touches on war-related mental functioning. Furthermore, they
may not wish to disclose or discuss their past or present psychological health
and despite the potential benefits of doing so. Therefore, medical and
para-medical personnel may fail to attach importance to the longterm effects of
participation in the KW when undertaking older veterans’ histories and
assessments.
Conclusion
and Recommendations
In
meeting the three objectives for this article, the use of life losses and gains
scales in conjunction with the CES and IES is an efficient way of gaining
insight into the extent and nature of the KW’s life-span effects and the
differences between combatants’ with non-combatants’ perspectives. As
participation in combat was not the sole causal agent of psychological distress
in this participant sample, it is recommended that greater attention should be
given to the non-combat conditions of a warzone as well as those of combat.
Further research is needed to establish whether this phenomenon is peculiar to
the KW (thus adding credence to its veterans’ belief that they are indeed
‘different from other wars’ veterans) or to veterans of all wars.
For
more Bio
statistics and Bio metrics Open Access Journal articles
Please Click Here: https://lupinepublishers.com/biostatistics-biometrics-journal/



No comments:
Post a Comment